Patients underwent upper endoscopy with examination of the esophagus, stomach, and duodenum (first and second portions). The cause is often not clear. 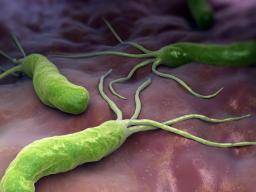 When the dyspepsia score was analyzed according to whether or not H pylori was successfully eradicated, those patients with persistent H pylori infection (40144, 65142, 45138, and 39163) actually demonstrated a better, but nonsignificant, clinical response than those in whom H pylori was successfully eradicated (26126, 26148, 12126, and 25151). Factors that can increase the risk of functional or non-ulcer dyspepsia include: Signs and symptoms of functional or non-ulcer dyspepsia may include: Your doctor will likely review your signs and symptoms and perform a physical examination. Silverstein
Soll
As our understanding of the pathogenesis of H pylori infection improves, it may be possible to select appropriate patients with nonulcer dyspepsia for H pylori treatment, based on the presence or absence of bacterial virulence factors.30. Hi, I was wondering if anyone experienced muscle twitching after stopping Omeprazole? 2022. Book a private assessment with a qualified dietician today. That is, other causes for dyspepsia such as duodenal ulcer, stomach ulcer, acid reflux and oesophagitis, inflamed stomach (gastritis) and eosinophilic oesophagitis are not the cause. MVYap
In the actively treated group, 95.2% of the omeprazole capsules were consumed, compared with 100% of the capsules in the placebo group (P=.07), and an estimated 94.5% of the clarithromycin tablets were ingested, compared with 99.5% of the tablets in the placebo group (P=.06). Follow-up upper endoscopy with biopsy was performed 4 weeks after treatment. Treatment of nonulcer dyspepsia can be challenging because of the need to balance medical management strategies with treatments for psychologic or functional disease. The blot was washed 3 times, and the color was developed by substrate solution (nitroblue tetrazolium reduction plus 5-bromo-4-chloro-3-indolyl phosphate [BCIP]) for 15 minutes. You may opt-out of email communications at any time by clicking on JFullerton
Helicobacter pylori infection. et al. CDe Reuck
Some experts advocate noninvasive serological testing for H pylori in patients with dyspepsia, followed by treatment of those whose test results are positive.20 Others recommend immediate upper endoscopy so that the cause of the dyspepsia can be determined from the outset.3 Because approximately 60% of patients with dyspepsia have nonulcer dyspepsia,2,3 the optimal approach in cases of dyspepsia may largely rest on whether or not treatment for H pylori in patients with nonulcer dyspepsia is beneficial. In this test a doctor looks inside your stomach and first part of your small intestine (the duodenum) by passing a thin, flexible telescope down your gullet (oesophagus). For details see our conditions. Furthermore, treatment of patients with nonulcer dyspepsia can be challenging because of the need to balance medical management strategies (e.g., eradication of Helicobacter pylori) with treatments for psychologic or functional disease. Although this approach may appear attractive from a management standpoint, it must be recognized that this strategy should lead to improvement in those patients with peptic ulcer disease (approximately 20% of patients with dyspepsia), but would not be likely to improve symptoms in the 80% of dyspeptic patients with nonulcer dyspepsia, acid-reflux disease, or gastric cancer. PD
Patients with nonulcer dyspepsia frequently are treated with tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), and anxiolytic agents. A number of diagnostic tests may help your doctor determine the cause of your discomfort. Our study demonstrates that treatment for H pylori is no better than placebo in improving symptoms in patients with nonulcer dyspepsia. However, we used clinical and endoscopic criteria to carefully exclude patients with predominant reflux symptoms or other definable diseases such as irritable bowel. CYLong-term outcome of triple therapy in. Most people with H. pylori infection will never have any signs or symptoms. Two biopsy specimens were obtained from both the antrum and the body of the stomach. Merck Manual Professional Version. Make a donation. Duodenal ulcer treated with, Santander
If you develop signs and symptoms of a peptic ulcer, your health care provider will probably test you for H. pylori infection.
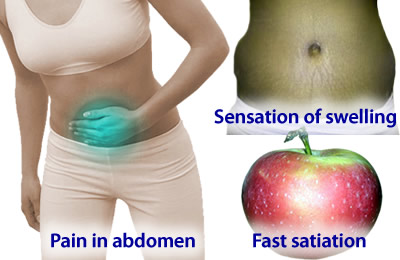
When the dyspepsia score was analyzed according to whether or not H pylori was successfully eradicated, those patients with persistent H pylori infection (40144, 65142, 45138, and 39163) actually demonstrated a better, but nonsignificant, clinical response than those in whom H pylori was successfully eradicated (26126, 26148, 12126, and 25151). Factors that can increase the risk of functional or non-ulcer dyspepsia include: Signs and symptoms of functional or non-ulcer dyspepsia may include: Your doctor will likely review your signs and symptoms and perform a physical examination. Silverstein
Soll
As our understanding of the pathogenesis of H pylori infection improves, it may be possible to select appropriate patients with nonulcer dyspepsia for H pylori treatment, based on the presence or absence of bacterial virulence factors.30. Hi, I was wondering if anyone experienced muscle twitching after stopping Omeprazole? 2022. Book a private assessment with a qualified dietician today. That is, other causes for dyspepsia such as duodenal ulcer, stomach ulcer, acid reflux and oesophagitis, inflamed stomach (gastritis) and eosinophilic oesophagitis are not the cause. MVYap
In the actively treated group, 95.2% of the omeprazole capsules were consumed, compared with 100% of the capsules in the placebo group (P=.07), and an estimated 94.5% of the clarithromycin tablets were ingested, compared with 99.5% of the tablets in the placebo group (P=.06). Follow-up upper endoscopy with biopsy was performed 4 weeks after treatment. Treatment of nonulcer dyspepsia can be challenging because of the need to balance medical management strategies with treatments for psychologic or functional disease. The blot was washed 3 times, and the color was developed by substrate solution (nitroblue tetrazolium reduction plus 5-bromo-4-chloro-3-indolyl phosphate [BCIP]) for 15 minutes. You may opt-out of email communications at any time by clicking on JFullerton
Helicobacter pylori infection. et al. CDe Reuck
Some experts advocate noninvasive serological testing for H pylori in patients with dyspepsia, followed by treatment of those whose test results are positive.20 Others recommend immediate upper endoscopy so that the cause of the dyspepsia can be determined from the outset.3 Because approximately 60% of patients with dyspepsia have nonulcer dyspepsia,2,3 the optimal approach in cases of dyspepsia may largely rest on whether or not treatment for H pylori in patients with nonulcer dyspepsia is beneficial. In this test a doctor looks inside your stomach and first part of your small intestine (the duodenum) by passing a thin, flexible telescope down your gullet (oesophagus). For details see our conditions. Furthermore, treatment of patients with nonulcer dyspepsia can be challenging because of the need to balance medical management strategies (e.g., eradication of Helicobacter pylori) with treatments for psychologic or functional disease. Although this approach may appear attractive from a management standpoint, it must be recognized that this strategy should lead to improvement in those patients with peptic ulcer disease (approximately 20% of patients with dyspepsia), but would not be likely to improve symptoms in the 80% of dyspeptic patients with nonulcer dyspepsia, acid-reflux disease, or gastric cancer. PD
Patients with nonulcer dyspepsia frequently are treated with tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), and anxiolytic agents. A number of diagnostic tests may help your doctor determine the cause of your discomfort. Our study demonstrates that treatment for H pylori is no better than placebo in improving symptoms in patients with nonulcer dyspepsia. However, we used clinical and endoscopic criteria to carefully exclude patients with predominant reflux symptoms or other definable diseases such as irritable bowel. CYLong-term outcome of triple therapy in. Most people with H. pylori infection will never have any signs or symptoms. Two biopsy specimens were obtained from both the antrum and the body of the stomach. Merck Manual Professional Version. Make a donation. Duodenal ulcer treated with, Santander
If you develop signs and symptoms of a peptic ulcer, your health care provider will probably test you for H. pylori infection.  DLZinmeister
At present, there is no way to determine which, if any, of these patients should be treated for H pylori.29 Preliminary evidence suggests that the presence of CagA in patients with H pylori infection predicts a more virulent strain that is more likely to lead to dyspeptic symptoms and ulcer disease than are strains without CagA.30 However, subset analysis of CagA status did not influence the main results of this study. The possibility remains that some patients were included in the present study and were inappropriately classified as having nonulcer dyspepsia, although this problem is not unique to our study. TPursey
Values are expressed as meanSD. Also, when embracing this strategy, one must take into consideration the possible adverse effects of antibiotic therapy as well as issues of drug resistance. For functional or non-ulcer dyspepsia, some basic questions to ask your doctor include: In addition to the questions that youve prepared to ask your doctor, dont hesitate to ask questions during your appointment at any time that you dont understand something. The mean score for each symptom during the 3-day period was recorded for each patient. Patients with predominant nausea and bloating may have motility dysfunction and may benefit from treatment with a promotility agent. The endoscopic appearance of the stomach and duodenum was scored separately based on modified criteria of Lanza27 (0, normal; 1, a single affected area with erythema or superficial erosion; 2, between 2 and 10 affected areas; 3, between 10 and 25 affected areas; 4, more than 25 affected areas; and 5, frank ulceration). CUzoechina
Patients with peptic ulcer disease, esophagitis, hepatobiliary disease, irritable bowel disease, or predominantly reflux-related symptoms were excluded by history and upper endoscopy. Allowing for a dropout rate of approximately 10%, we enrolled 50 patients in each arm of this study. Mayo Clinic. What are the alternatives to the primary approach that youre suggesting? et al. For each symptom, a score ranging from 0 to 100 was recorded daily over 3 consecutive days. Results
JMSchaffalitzky de Muchadell
However, as mentioned, infection with H. pylori is probably a coincidence rather than a cause in most cases of non-ulcer dyspepsia. AskMayoExpert. To provide you with the most relevant and helpful information, and understand which 2022 American Medical Association. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. Prior studies have yielded conflicting results on whether or not Helicobacter pylori causes nonulcer dyspepsia. Pathogenesis and clinical management of Helicobacter pylori gastric infection. JJChung
ALabbe
DLZinmeister
At present, there is no way to determine which, if any, of these patients should be treated for H pylori.29 Preliminary evidence suggests that the presence of CagA in patients with H pylori infection predicts a more virulent strain that is more likely to lead to dyspeptic symptoms and ulcer disease than are strains without CagA.30 However, subset analysis of CagA status did not influence the main results of this study. The possibility remains that some patients were included in the present study and were inappropriately classified as having nonulcer dyspepsia, although this problem is not unique to our study. TPursey
Values are expressed as meanSD. Also, when embracing this strategy, one must take into consideration the possible adverse effects of antibiotic therapy as well as issues of drug resistance. For functional or non-ulcer dyspepsia, some basic questions to ask your doctor include: In addition to the questions that youve prepared to ask your doctor, dont hesitate to ask questions during your appointment at any time that you dont understand something. The mean score for each symptom during the 3-day period was recorded for each patient. Patients with predominant nausea and bloating may have motility dysfunction and may benefit from treatment with a promotility agent. The endoscopic appearance of the stomach and duodenum was scored separately based on modified criteria of Lanza27 (0, normal; 1, a single affected area with erythema or superficial erosion; 2, between 2 and 10 affected areas; 3, between 10 and 25 affected areas; 4, more than 25 affected areas; and 5, frank ulceration). CUzoechina
Patients with peptic ulcer disease, esophagitis, hepatobiliary disease, irritable bowel disease, or predominantly reflux-related symptoms were excluded by history and upper endoscopy. Allowing for a dropout rate of approximately 10%, we enrolled 50 patients in each arm of this study. Mayo Clinic. What are the alternatives to the primary approach that youre suggesting? et al. For each symptom, a score ranging from 0 to 100 was recorded daily over 3 consecutive days. Results
JMSchaffalitzky de Muchadell
However, as mentioned, infection with H. pylori is probably a coincidence rather than a cause in most cases of non-ulcer dyspepsia. AskMayoExpert. To provide you with the most relevant and helpful information, and understand which 2022 American Medical Association. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. Prior studies have yielded conflicting results on whether or not Helicobacter pylori causes nonulcer dyspepsia. Pathogenesis and clinical management of Helicobacter pylori gastric infection. JJChung
ALabbe
 et al. Bittencourt de Brito B, et al. Epub 2016 Apr 28. Patients meeting inclusion and exclusion criteria were randomized to 2 weeks of treatment with omeprazole (Prilosec) (20 mg twice daily) and clarithromycin (Biaxin) (500 mg three times daily) or with identical-appearing placebos in a double-blind manner.
et al. Bittencourt de Brito B, et al. Epub 2016 Apr 28. Patients meeting inclusion and exclusion criteria were randomized to 2 weeks of treatment with omeprazole (Prilosec) (20 mg twice daily) and clarithromycin (Biaxin) (500 mg three times daily) or with identical-appearing placebos in a double-blind manner.  How can I best manage them together? All patients had the opportunity to ask questions about the study, and signed informed consent was obtained at the time of enrollment. Advertising revenue supports our not-for-profit mission. On these tests, 25 to 60 percent of patients with nonulcer dyspepsia exhibit motility dysfunction.8,9, Symptoms of nonulcer dyspepsia correlate poorly with regional gastric-emptying problems such as decreased compliance in the proximal stomach and relaxation of the distal end.10 Patients may or may not improve when they are given promotility agents; sometimes motility improves, but the symptoms of nonulcer dyspepsia do not.11, Motor dysfunction involving the gall-bladder and biliary tract may play a role in nonulcer dyspepsia. Aust Prescr.
How can I best manage them together? All patients had the opportunity to ask questions about the study, and signed informed consent was obtained at the time of enrollment. Advertising revenue supports our not-for-profit mission. On these tests, 25 to 60 percent of patients with nonulcer dyspepsia exhibit motility dysfunction.8,9, Symptoms of nonulcer dyspepsia correlate poorly with regional gastric-emptying problems such as decreased compliance in the proximal stomach and relaxation of the distal end.10 Patients may or may not improve when they are given promotility agents; sometimes motility improves, but the symptoms of nonulcer dyspepsia do not.11, Motor dysfunction involving the gall-bladder and biliary tract may play a role in nonulcer dyspepsia. Aust Prescr. 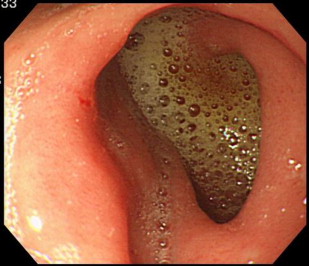 OMaconi
The prominent symptom for enrolled patients was a dull ache or pain located predominantly in the upper midabdominal area. Furthermore, within the actively treated group, the CagA-positive patients (38128, 29147, 10147, and 7133) and the CagA-negative patients (22120, 79132, 3718, and 129138) with successful H pylori eradication had a similar improvement in mean dyspepsia scores. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions. Diseases of the stomach and duodenum. MBargiggia
JPajares
JAVan Spreeuwel
Addressing only one factor, such as H. pylori infection or motility dysfunction, is unlikely to be successful and may be frustrating for the patient and the physician. If you have a runny nose/congestion, sore throat, fever, cough or shortness of breath or have been in contact with a person who has or might have COVID-19, please call the clinic before coming to your appointment.
OMaconi
The prominent symptom for enrolled patients was a dull ache or pain located predominantly in the upper midabdominal area. Furthermore, within the actively treated group, the CagA-positive patients (38128, 29147, 10147, and 7133) and the CagA-negative patients (22120, 79132, 3718, and 129138) with successful H pylori eradication had a similar improvement in mean dyspepsia scores. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions. Diseases of the stomach and duodenum. MBargiggia
JPajares
JAVan Spreeuwel
Addressing only one factor, such as H. pylori infection or motility dysfunction, is unlikely to be successful and may be frustrating for the patient and the physician. If you have a runny nose/congestion, sore throat, fever, cough or shortness of breath or have been in contact with a person who has or might have COVID-19, please call the clinic before coming to your appointment. 
.jpg.aspx) These data argue strongly that H pylori is not a cause of nonulcer dyspepsia in most patients infected with the organism. information submitted for this request. BSommer
MKorman
2017; doi:10.1038/ajg.2016.563. What are other possible causes for my stomach pain? Upgrade to Patient Pro Medical Professional? Prokinetic agents often are touted as the most effective medications for the management of nonulcer dyspepsia. Overall, psychotherapy should be reserved for use in patients with a significant comorbid psychiatric condition or as an adjunct to medical management. The presence or absence of H pylori was determined using hematoxylin-eosin stains. Therefore, these medications should be initiated at the lowest dosage, and the dosage should be increased slowly. Accessed Jan. 31, 2022. Infection with Helicobacter pylori (H. pylori) may cause a small number of cases. We used a treatment regimen that specifically did not include bismuth, given the difficulty in establishing secure patient blinding with bismuth. GHScheiman
Accessibility Statement, Our website uses cookies to enhance your experience. Patients whose symptoms were primarily reflux related (eg, heartburn) were not enrolled. The symptoms seem to come from the upper gut but the cause is not known. BTrapp
Patients were ineligible if gastric or duodenal ulcers were present (defined as a mucosal defect at least 2 mm in length with perceived depth), although patients with erosions alone were eligible. Non-ulcer dyspepsia causes pain and sometimes other symptoms in your upper tummy (abdomen). B
MDeprez
Patients in both groups were equally likely to have taken histamine2-receptor antagonists or proton pump inhibitors throughout the study period. Eradication was more successful in the compliant patients (23/29, 79%) than in the noncompliant patients or in those for whom tablet counts could not be verified (8/15, 53%) (P=.09). 1999;159(19):22832288. Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health. This site complies with the HONcode standard for trustworthy health information: verify here. A one-month trial of medication that reduces stomach acid is often advised. American College of Gastroenterology. Feb. 5, 2022. Doctors consider it a functional disorder, which means its not necessarily caused by a specific disease. MPorro
A side-effect of some medicines can cause dyspepsia: There are various other medicines which sometimes cause dyspepsia, or make dyspepsia worse. Mean dyspepsia scores. The combination of psychologic symptoms, motility dysfunction, infection, and nonulcer dyspepsia may be best understood as a complex interaction of factors. Some people feel that certain foods and drinks may cause the symptoms or make them worse. EKeane
Among the CagA-positive patients, there was no difference in the change in dyspepsia score between those with successful eradication (27131, 25143, 5142, and 3145) and those with persistent infection (50145, 81137, 53141, and 47151) at any time. MLonardo
BSLin
AGuan
Patient meets the following criteria for at least 12 weeks (which need not be consecutive) within the preceding 12 months: Persistent or recurrent symptoms (pain or discomfort centered in the upper abdomen), No evidence of organic disease (including on upper endoscopy) that is likely to explain the symptoms, No evidence that dyspepsia is relieved exclusively by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel syndrome), Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow), Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 enzyme inhibitors. To prepare for your appointment, try to: Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. 2021; doi:10.3389/fmicb.2021.630852. Presented in part at the annual meeting of the American Gastroenterological Association, San Francisco, Calif, May 19-22, 1996. The change in dyspepsia score was calculated by taking the difference in the score at baseline from the score at 1, 3, 6, and 12 months (negative changes in the dyspepsia score indicated improved symptoms, while positive changes indicated worsened symptoms). Both H pylori infection and dyspepsia are common, and many patients with dyspepsia are infected with H pylori. Chey WD, et al. Accessed Jan. 31, 2022. If you have non-ulcer dyspepsia, the inside of your gut looks normal. This content does not have an English version. TTalley
The cause of irritable bowel syndrome is not known. However, at one year, the improvement in symptoms was not statistically significant in two of the studies.20 [SOR B, inconsistent findings from RCTs] Results from these studies were not combined because the interventions were quite different. Establishing the diagnosis of peptic or duodenal ulcer greatly clarifies the treatment approach. Peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer must be excluded. CDMelton
CO'Morain
Accessed Jan. 31, 2022. Non-ulcer stomach pain can cause signs and symptoms that resemble those of an ulcer, such as pain or discomfort in your upper abdomen, often accompanied by bloating, belching and nausea. All Rights Reserved. When signs or symptoms do occur with H. pylori infection, they are typically related to gastritis or a peptic ulcer and may include: Make an appointment with your health care provider if you notice any signs and symptoms that may be gastritis or a peptic ulcer. Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press. The amount of acid in the stomach is normal. Epub 2017 Dec 4. ARSchleck
Seek immediate medical help if you have: There is a problem with The following are some theories as to possible causes: Strictly speaking, non-ulcer dyspepsia is a diagnosis that is made only when no other cause can be found for the symptoms (such as an ulcer). Prior to enrollment, patients had been referred to the gastrointestinal clinic for evaluation at San Francisco General Hospital, San Francisco, Calif. See permissionsforcopyrightquestions and/or permission requests. National Institute of Diabetes and Digestive and Kidney Diseases. Helicobacter pylori (adult). Studies have shown that symptomatic improvement is 45 to 50 percent greater with cisapride, domperidone, or metoclopramide therapy than with placebo.4,28 [Reference 28: SOR A, systematic review of limited-quality studies] However, the studies have been of poor quality. An ache or burning pain in your stomach (abdomen), Stomach pain that may be worse when your stomach is empty, Severe or ongoing stomach (abdominal) pain that may awaken you from sleep, Bloody or black vomit or vomit that looks like coffee grounds. A 2 test with a Fisher exact test was used for comparison between proportional data.28 All tests were 2-tailed, and P values less than .05 were considered statistically significant. For every 15 patients with nonulcer dyspepsia in whom H. pylori is eradicated, one fewer patient has dyspepsia a year later.32 [SOR B, systematic review of inconsistent or limited-quality studies] Another study found a small increase (7 percent) in the likelihood of treatment success with H. pylori eradication.33 [SOR B, systematic review of inconsistent or limited-quality studies], More studies are needed to resolve the conflicting study results and to determine whether, as some investigators claim, a modest benefit for H. pylori eradication may be cost-effective.31 Eradication regimens are reviewed elsewhere.34. Three (8%) of 40 patients in the placebo group and 31 (71%) of 44 patients in the omeprazole and clarithromycin group had complete eradication of H pylori (P<.001). Peptic ulcer disease. H. pylori may also be spread through contaminated food or water. The muscles in the stomach wall may not work as well as they should. Patients and Methods
All Rights Reserved. Pain that radiates to your jaw, neck or arm. Continuous variables are presented as meanSD. CLong-term prospective study of, Lazzaroni
A test to detect the H. pylori germ (bacterium) may be done. Functional or non-ulcer dyspepsia is common and can be long-lasting. A more recent article on functional dyspepsia is available. All Rights Reserved. B
The groups were well matched for demographic and laboratory parameters, with the exception of a higher mean serum alanine aminotransferase level in the actively treated group (Table 1). To explain the symptoms of nonulcer dyspepsia more fully, researchers have focused on several key factors: motility disorders, nonmotility disorders (including H. pylori infection), and psychosocial factors. Risk factors for H. pylori infection are related to living conditions in childhood, such as: A peptic ulcer is a sore on the lining of your stomach, small intestine or esophagus. WLThe treatment of. Your doctor may recommend lifestyle changes to help you control your functional or non-ulcer dyspepsia. Furthermore, patients with persistent, Patients with nonulcer dyspepsia should not routinely be treated for. information and will only use or disclose that information as set forth in our notice of In general, the trials included patients with documented H. pylori infection, used typical dual or triple therapy for H. pylori infection (i.e., antisecretory therapy plus antibiotics), and evaluated dyspepsia at three and 12 months. The guidelines outlined in the Maastricht European consensus report25 recommend endoscopy for patients older than 45 years, whereas the American Digestive Health Foundation26 recommends endoscopy for patients with dyspepsia who are older than 50 years. Effect of treatment of, Sung
In the present study, we enrolled patients in whom an empiric trial of a histamine2-receptor antagonist had failed and in whom peptic ulcer disease and gastroesophageal reflux disease had been excluded. DYLew
These data argue strongly that H pylori is not a cause of nonulcer dyspepsia in most patients infected with the organism. information submitted for this request. BSommer
MKorman
2017; doi:10.1038/ajg.2016.563. What are other possible causes for my stomach pain? Upgrade to Patient Pro Medical Professional? Prokinetic agents often are touted as the most effective medications for the management of nonulcer dyspepsia. Overall, psychotherapy should be reserved for use in patients with a significant comorbid psychiatric condition or as an adjunct to medical management. The presence or absence of H pylori was determined using hematoxylin-eosin stains. Therefore, these medications should be initiated at the lowest dosage, and the dosage should be increased slowly. Accessed Jan. 31, 2022. Infection with Helicobacter pylori (H. pylori) may cause a small number of cases. We used a treatment regimen that specifically did not include bismuth, given the difficulty in establishing secure patient blinding with bismuth. GHScheiman
Accessibility Statement, Our website uses cookies to enhance your experience. Patients whose symptoms were primarily reflux related (eg, heartburn) were not enrolled. The symptoms seem to come from the upper gut but the cause is not known. BTrapp
Patients were ineligible if gastric or duodenal ulcers were present (defined as a mucosal defect at least 2 mm in length with perceived depth), although patients with erosions alone were eligible. Non-ulcer dyspepsia causes pain and sometimes other symptoms in your upper tummy (abdomen). B
MDeprez
Patients in both groups were equally likely to have taken histamine2-receptor antagonists or proton pump inhibitors throughout the study period. Eradication was more successful in the compliant patients (23/29, 79%) than in the noncompliant patients or in those for whom tablet counts could not be verified (8/15, 53%) (P=.09). 1999;159(19):22832288. Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health. This site complies with the HONcode standard for trustworthy health information: verify here. A one-month trial of medication that reduces stomach acid is often advised. American College of Gastroenterology. Feb. 5, 2022. Doctors consider it a functional disorder, which means its not necessarily caused by a specific disease. MPorro
A side-effect of some medicines can cause dyspepsia: There are various other medicines which sometimes cause dyspepsia, or make dyspepsia worse. Mean dyspepsia scores. The combination of psychologic symptoms, motility dysfunction, infection, and nonulcer dyspepsia may be best understood as a complex interaction of factors. Some people feel that certain foods and drinks may cause the symptoms or make them worse. EKeane
Among the CagA-positive patients, there was no difference in the change in dyspepsia score between those with successful eradication (27131, 25143, 5142, and 3145) and those with persistent infection (50145, 81137, 53141, and 47151) at any time. MLonardo
BSLin
AGuan
Patient meets the following criteria for at least 12 weeks (which need not be consecutive) within the preceding 12 months: Persistent or recurrent symptoms (pain or discomfort centered in the upper abdomen), No evidence of organic disease (including on upper endoscopy) that is likely to explain the symptoms, No evidence that dyspepsia is relieved exclusively by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel syndrome), Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow), Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 enzyme inhibitors. To prepare for your appointment, try to: Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. 2021; doi:10.3389/fmicb.2021.630852. Presented in part at the annual meeting of the American Gastroenterological Association, San Francisco, Calif, May 19-22, 1996. The change in dyspepsia score was calculated by taking the difference in the score at baseline from the score at 1, 3, 6, and 12 months (negative changes in the dyspepsia score indicated improved symptoms, while positive changes indicated worsened symptoms). Both H pylori infection and dyspepsia are common, and many patients with dyspepsia are infected with H pylori. Chey WD, et al. Accessed Jan. 31, 2022. If you have non-ulcer dyspepsia, the inside of your gut looks normal. This content does not have an English version. TTalley
The cause of irritable bowel syndrome is not known. However, at one year, the improvement in symptoms was not statistically significant in two of the studies.20 [SOR B, inconsistent findings from RCTs] Results from these studies were not combined because the interventions were quite different. Establishing the diagnosis of peptic or duodenal ulcer greatly clarifies the treatment approach. Peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer must be excluded. CDMelton
CO'Morain
Accessed Jan. 31, 2022. Non-ulcer stomach pain can cause signs and symptoms that resemble those of an ulcer, such as pain or discomfort in your upper abdomen, often accompanied by bloating, belching and nausea. All Rights Reserved. When signs or symptoms do occur with H. pylori infection, they are typically related to gastritis or a peptic ulcer and may include: Make an appointment with your health care provider if you notice any signs and symptoms that may be gastritis or a peptic ulcer. Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press. The amount of acid in the stomach is normal. Epub 2017 Dec 4. ARSchleck
Seek immediate medical help if you have: There is a problem with The following are some theories as to possible causes: Strictly speaking, non-ulcer dyspepsia is a diagnosis that is made only when no other cause can be found for the symptoms (such as an ulcer). Prior to enrollment, patients had been referred to the gastrointestinal clinic for evaluation at San Francisco General Hospital, San Francisco, Calif. See permissionsforcopyrightquestions and/or permission requests. National Institute of Diabetes and Digestive and Kidney Diseases. Helicobacter pylori (adult). Studies have shown that symptomatic improvement is 45 to 50 percent greater with cisapride, domperidone, or metoclopramide therapy than with placebo.4,28 [Reference 28: SOR A, systematic review of limited-quality studies] However, the studies have been of poor quality. An ache or burning pain in your stomach (abdomen), Stomach pain that may be worse when your stomach is empty, Severe or ongoing stomach (abdominal) pain that may awaken you from sleep, Bloody or black vomit or vomit that looks like coffee grounds. A 2 test with a Fisher exact test was used for comparison between proportional data.28 All tests were 2-tailed, and P values less than .05 were considered statistically significant. For every 15 patients with nonulcer dyspepsia in whom H. pylori is eradicated, one fewer patient has dyspepsia a year later.32 [SOR B, systematic review of inconsistent or limited-quality studies] Another study found a small increase (7 percent) in the likelihood of treatment success with H. pylori eradication.33 [SOR B, systematic review of inconsistent or limited-quality studies], More studies are needed to resolve the conflicting study results and to determine whether, as some investigators claim, a modest benefit for H. pylori eradication may be cost-effective.31 Eradication regimens are reviewed elsewhere.34. Three (8%) of 40 patients in the placebo group and 31 (71%) of 44 patients in the omeprazole and clarithromycin group had complete eradication of H pylori (P<.001). Peptic ulcer disease. H. pylori may also be spread through contaminated food or water. The muscles in the stomach wall may not work as well as they should. Patients and Methods
All Rights Reserved. Pain that radiates to your jaw, neck or arm. Continuous variables are presented as meanSD. CLong-term prospective study of, Lazzaroni
A test to detect the H. pylori germ (bacterium) may be done. Functional or non-ulcer dyspepsia is common and can be long-lasting. A more recent article on functional dyspepsia is available. All Rights Reserved. B
The groups were well matched for demographic and laboratory parameters, with the exception of a higher mean serum alanine aminotransferase level in the actively treated group (Table 1). To explain the symptoms of nonulcer dyspepsia more fully, researchers have focused on several key factors: motility disorders, nonmotility disorders (including H. pylori infection), and psychosocial factors. Risk factors for H. pylori infection are related to living conditions in childhood, such as: A peptic ulcer is a sore on the lining of your stomach, small intestine or esophagus. WLThe treatment of. Your doctor may recommend lifestyle changes to help you control your functional or non-ulcer dyspepsia. Furthermore, patients with persistent, Patients with nonulcer dyspepsia should not routinely be treated for. information and will only use or disclose that information as set forth in our notice of In general, the trials included patients with documented H. pylori infection, used typical dual or triple therapy for H. pylori infection (i.e., antisecretory therapy plus antibiotics), and evaluated dyspepsia at three and 12 months. The guidelines outlined in the Maastricht European consensus report25 recommend endoscopy for patients older than 45 years, whereas the American Digestive Health Foundation26 recommends endoscopy for patients with dyspepsia who are older than 50 years. Effect of treatment of, Sung
In the present study, we enrolled patients in whom an empiric trial of a histamine2-receptor antagonist had failed and in whom peptic ulcer disease and gastroesophageal reflux disease had been excluded. DYLew
 JHPeterson
The studied interventions included psychotherapy, psychodrama, cognitive behavior therapy, relaxation therapy, and guided imagery or hypnosis.
JHPeterson
The studied interventions included psychotherapy, psychodrama, cognitive behavior therapy, relaxation therapy, and guided imagery or hypnosis.  Copyright 2022 American Academy of Family Physicians. The dyspepsia score was calculated by summing the mean scores for 5 symptoms (nausea, abdominal pain, abdominal bloating, abdominal burning, and pain after eating). 2019; doi:10.3748/wjg.v25.i37.5578. Therefore, H2RAs are preferred, because of their lower cost.28 One review4 noted that most studies have used higher H2RA dosages than those available in over-the-counter formulations, with improvement occurring in approximately 25 percent more patients treated with H2RAs compared with placebo. Not surprisingly, nonulcer dyspepsia is responsible for substantial costs to the U.S. health care system (direct medical costs) and to society (e.g., lost time from work, diminished work productivity).6 A better understanding of this condition and its management can improve patient care and decrease unnecessary medical expenditures. Stress from life events also has been correlated with these symptoms and has been linked to exacerbations of nonulcer dyspepsia.1 In addition, the condition has been linked to the symptoms of irritable bowel syndrome (despite the emphasis on lower versus upper gastrointestinal tract symptoms), an illness known to be connected to stress.21. Kang
What are the treatment options for non-ulcer dyspepsia? information highlighted below and resubmit the form. You may also learn ways to reduce stress in your life in order to prevent functional or non-ulcer dyspepsia from recurring. The diagnosis of dyspepsia is challenging because patients often exhibit changing symptoms, and because characterization of the symptoms provides little information about the nature of the underlying physiologic abnormality.22,23. What treatment you receive depends on your signs and symptoms. A popular, although unproved, management strategy has been to screen dyspeptic patients with a serum enzyme-linked immunosorbent assay for H pylori.31-33 Patients with positive results are then treated for H pylori and are followed up clinically. All rights reserved. An organic cause, such as duodenal ulcer, is found in only about 40 percent of these patients.1 Hence, dyspepsia is considered to be functional, or idiopathic, in as many as 60 percent of patients (Table 1).24 The Rome II criteria provide an updated definition of nonulcer dyspepsia (Table 2).5 Symptoms usually are categorized as ulcer-like (i.e., burning sensation, relief with antacids and histamine-H2 blockers or proton pump inhibitors), dysmotility-like (i.e., nausea, bloating, early satiety, anorexia), or unspecified.5. People often get H. pylori infection during childhood. Because eradication of H pylori in patients with peptic ulcer disease successfully reduces the recurrence of ulcers and improves symptoms,21-26 it is possible that eradication of H pylori will similarly improve symptoms in patients with nonulcer dyspepsia. information is beneficial, we may combine your email and website usage information with I have these other health conditions.
Copyright 2022 American Academy of Family Physicians. The dyspepsia score was calculated by summing the mean scores for 5 symptoms (nausea, abdominal pain, abdominal bloating, abdominal burning, and pain after eating). 2019; doi:10.3748/wjg.v25.i37.5578. Therefore, H2RAs are preferred, because of their lower cost.28 One review4 noted that most studies have used higher H2RA dosages than those available in over-the-counter formulations, with improvement occurring in approximately 25 percent more patients treated with H2RAs compared with placebo. Not surprisingly, nonulcer dyspepsia is responsible for substantial costs to the U.S. health care system (direct medical costs) and to society (e.g., lost time from work, diminished work productivity).6 A better understanding of this condition and its management can improve patient care and decrease unnecessary medical expenditures. Stress from life events also has been correlated with these symptoms and has been linked to exacerbations of nonulcer dyspepsia.1 In addition, the condition has been linked to the symptoms of irritable bowel syndrome (despite the emphasis on lower versus upper gastrointestinal tract symptoms), an illness known to be connected to stress.21. Kang
What are the treatment options for non-ulcer dyspepsia? information highlighted below and resubmit the form. You may also learn ways to reduce stress in your life in order to prevent functional or non-ulcer dyspepsia from recurring. The diagnosis of dyspepsia is challenging because patients often exhibit changing symptoms, and because characterization of the symptoms provides little information about the nature of the underlying physiologic abnormality.22,23. What treatment you receive depends on your signs and symptoms. A popular, although unproved, management strategy has been to screen dyspeptic patients with a serum enzyme-linked immunosorbent assay for H pylori.31-33 Patients with positive results are then treated for H pylori and are followed up clinically. All rights reserved. An organic cause, such as duodenal ulcer, is found in only about 40 percent of these patients.1 Hence, dyspepsia is considered to be functional, or idiopathic, in as many as 60 percent of patients (Table 1).24 The Rome II criteria provide an updated definition of nonulcer dyspepsia (Table 2).5 Symptoms usually are categorized as ulcer-like (i.e., burning sensation, relief with antacids and histamine-H2 blockers or proton pump inhibitors), dysmotility-like (i.e., nausea, bloating, early satiety, anorexia), or unspecified.5. People often get H. pylori infection during childhood. Because eradication of H pylori in patients with peptic ulcer disease successfully reduces the recurrence of ulcers and improves symptoms,21-26 it is possible that eradication of H pylori will similarly improve symptoms in patients with nonulcer dyspepsia. information is beneficial, we may combine your email and website usage information with I have these other health conditions.  J, Rokkas
J, Rokkas


 If you are infected with H. pylori, the first treatment usually tried is to clear the H. pylori infection. YBurette
In 2 of these studies, however, there were only about 20 patients randomized to each study arm, with even fewer completing the study.5,6 Another study did not have a control group and had an extremely high reinfection rate, suggesting that H pylori was not truly eradicated.4 Most importantly, none of these 3 studies had a true untreated, placebo group, and none provided data on an intention-to-treat basis.
If you are infected with H. pylori, the first treatment usually tried is to clear the H. pylori infection. YBurette
In 2 of these studies, however, there were only about 20 patients randomized to each study arm, with even fewer completing the study.5,6 Another study did not have a control group and had an extremely high reinfection rate, suggesting that H pylori was not truly eradicated.4 Most importantly, none of these 3 studies had a true untreated, placebo group, and none provided data on an intention-to-treat basis.
When the dyspepsia score was analyzed according to whether or not H pylori was successfully eradicated, those patients with persistent H pylori infection (40144, 65142, 45138, and 39163) actually demonstrated a better, but nonsignificant, clinical response than those in whom H pylori was successfully eradicated (26126, 26148, 12126, and 25151). Factors that can increase the risk of functional or non-ulcer dyspepsia include: Signs and symptoms of functional or non-ulcer dyspepsia may include: Your doctor will likely review your signs and symptoms and perform a physical examination. Silverstein
Soll
As our understanding of the pathogenesis of H pylori infection improves, it may be possible to select appropriate patients with nonulcer dyspepsia for H pylori treatment, based on the presence or absence of bacterial virulence factors.30. Hi, I was wondering if anyone experienced muscle twitching after stopping Omeprazole? 2022. Book a private assessment with a qualified dietician today. That is, other causes for dyspepsia such as duodenal ulcer, stomach ulcer, acid reflux and oesophagitis, inflamed stomach (gastritis) and eosinophilic oesophagitis are not the cause. MVYap
In the actively treated group, 95.2% of the omeprazole capsules were consumed, compared with 100% of the capsules in the placebo group (P=.07), and an estimated 94.5% of the clarithromycin tablets were ingested, compared with 99.5% of the tablets in the placebo group (P=.06). Follow-up upper endoscopy with biopsy was performed 4 weeks after treatment. Treatment of nonulcer dyspepsia can be challenging because of the need to balance medical management strategies with treatments for psychologic or functional disease. The blot was washed 3 times, and the color was developed by substrate solution (nitroblue tetrazolium reduction plus 5-bromo-4-chloro-3-indolyl phosphate [BCIP]) for 15 minutes. You may opt-out of email communications at any time by clicking on JFullerton
Helicobacter pylori infection. et al. CDe Reuck
Some experts advocate noninvasive serological testing for H pylori in patients with dyspepsia, followed by treatment of those whose test results are positive.20 Others recommend immediate upper endoscopy so that the cause of the dyspepsia can be determined from the outset.3 Because approximately 60% of patients with dyspepsia have nonulcer dyspepsia,2,3 the optimal approach in cases of dyspepsia may largely rest on whether or not treatment for H pylori in patients with nonulcer dyspepsia is beneficial. In this test a doctor looks inside your stomach and first part of your small intestine (the duodenum) by passing a thin, flexible telescope down your gullet (oesophagus). For details see our conditions. Furthermore, treatment of patients with nonulcer dyspepsia can be challenging because of the need to balance medical management strategies (e.g., eradication of Helicobacter pylori) with treatments for psychologic or functional disease. Although this approach may appear attractive from a management standpoint, it must be recognized that this strategy should lead to improvement in those patients with peptic ulcer disease (approximately 20% of patients with dyspepsia), but would not be likely to improve symptoms in the 80% of dyspeptic patients with nonulcer dyspepsia, acid-reflux disease, or gastric cancer. PD
Patients with nonulcer dyspepsia frequently are treated with tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), and anxiolytic agents. A number of diagnostic tests may help your doctor determine the cause of your discomfort. Our study demonstrates that treatment for H pylori is no better than placebo in improving symptoms in patients with nonulcer dyspepsia. However, we used clinical and endoscopic criteria to carefully exclude patients with predominant reflux symptoms or other definable diseases such as irritable bowel. CYLong-term outcome of triple therapy in. Most people with H. pylori infection will never have any signs or symptoms. Two biopsy specimens were obtained from both the antrum and the body of the stomach. Merck Manual Professional Version. Make a donation. Duodenal ulcer treated with, Santander
If you develop signs and symptoms of a peptic ulcer, your health care provider will probably test you for H. pylori infection. DLZinmeister
At present, there is no way to determine which, if any, of these patients should be treated for H pylori.29 Preliminary evidence suggests that the presence of CagA in patients with H pylori infection predicts a more virulent strain that is more likely to lead to dyspeptic symptoms and ulcer disease than are strains without CagA.30 However, subset analysis of CagA status did not influence the main results of this study. The possibility remains that some patients were included in the present study and were inappropriately classified as having nonulcer dyspepsia, although this problem is not unique to our study. TPursey
Values are expressed as meanSD. Also, when embracing this strategy, one must take into consideration the possible adverse effects of antibiotic therapy as well as issues of drug resistance. For functional or non-ulcer dyspepsia, some basic questions to ask your doctor include: In addition to the questions that youve prepared to ask your doctor, dont hesitate to ask questions during your appointment at any time that you dont understand something. The mean score for each symptom during the 3-day period was recorded for each patient. Patients with predominant nausea and bloating may have motility dysfunction and may benefit from treatment with a promotility agent. The endoscopic appearance of the stomach and duodenum was scored separately based on modified criteria of Lanza27 (0, normal; 1, a single affected area with erythema or superficial erosion; 2, between 2 and 10 affected areas; 3, between 10 and 25 affected areas; 4, more than 25 affected areas; and 5, frank ulceration). CUzoechina
Patients with peptic ulcer disease, esophagitis, hepatobiliary disease, irritable bowel disease, or predominantly reflux-related symptoms were excluded by history and upper endoscopy. Allowing for a dropout rate of approximately 10%, we enrolled 50 patients in each arm of this study. Mayo Clinic. What are the alternatives to the primary approach that youre suggesting? et al. For each symptom, a score ranging from 0 to 100 was recorded daily over 3 consecutive days. Results
JMSchaffalitzky de Muchadell
However, as mentioned, infection with H. pylori is probably a coincidence rather than a cause in most cases of non-ulcer dyspepsia. AskMayoExpert. To provide you with the most relevant and helpful information, and understand which 2022 American Medical Association. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. Prior studies have yielded conflicting results on whether or not Helicobacter pylori causes nonulcer dyspepsia. Pathogenesis and clinical management of Helicobacter pylori gastric infection. JJChung
ALabbe
How can I best manage them together? All patients had the opportunity to ask questions about the study, and signed informed consent was obtained at the time of enrollment. Advertising revenue supports our not-for-profit mission. On these tests, 25 to 60 percent of patients with nonulcer dyspepsia exhibit motility dysfunction.8,9, Symptoms of nonulcer dyspepsia correlate poorly with regional gastric-emptying problems such as decreased compliance in the proximal stomach and relaxation of the distal end.10 Patients may or may not improve when they are given promotility agents; sometimes motility improves, but the symptoms of nonulcer dyspepsia do not.11, Motor dysfunction involving the gall-bladder and biliary tract may play a role in nonulcer dyspepsia. Aust Prescr. OMaconi
The prominent symptom for enrolled patients was a dull ache or pain located predominantly in the upper midabdominal area. Furthermore, within the actively treated group, the CagA-positive patients (38128, 29147, 10147, and 7133) and the CagA-negative patients (22120, 79132, 3718, and 129138) with successful H pylori eradication had a similar improvement in mean dyspepsia scores. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions. Diseases of the stomach and duodenum. MBargiggia
JPajares
JAVan Spreeuwel
Addressing only one factor, such as H. pylori infection or motility dysfunction, is unlikely to be successful and may be frustrating for the patient and the physician. If you have a runny nose/congestion, sore throat, fever, cough or shortness of breath or have been in contact with a person who has or might have COVID-19, please call the clinic before coming to your appointment. These data argue strongly that H pylori is not a cause of nonulcer dyspepsia in most patients infected with the organism. information submitted for this request. BSommer
MKorman
2017; doi:10.1038/ajg.2016.563. What are other possible causes for my stomach pain? Upgrade to Patient Pro Medical Professional? Prokinetic agents often are touted as the most effective medications for the management of nonulcer dyspepsia. Overall, psychotherapy should be reserved for use in patients with a significant comorbid psychiatric condition or as an adjunct to medical management. The presence or absence of H pylori was determined using hematoxylin-eosin stains. Therefore, these medications should be initiated at the lowest dosage, and the dosage should be increased slowly. Accessed Jan. 31, 2022. Infection with Helicobacter pylori (H. pylori) may cause a small number of cases. We used a treatment regimen that specifically did not include bismuth, given the difficulty in establishing secure patient blinding with bismuth. GHScheiman
Accessibility Statement, Our website uses cookies to enhance your experience. Patients whose symptoms were primarily reflux related (eg, heartburn) were not enrolled. The symptoms seem to come from the upper gut but the cause is not known. BTrapp
Patients were ineligible if gastric or duodenal ulcers were present (defined as a mucosal defect at least 2 mm in length with perceived depth), although patients with erosions alone were eligible. Non-ulcer dyspepsia causes pain and sometimes other symptoms in your upper tummy (abdomen). B
MDeprez
Patients in both groups were equally likely to have taken histamine2-receptor antagonists or proton pump inhibitors throughout the study period. Eradication was more successful in the compliant patients (23/29, 79%) than in the noncompliant patients or in those for whom tablet counts could not be verified (8/15, 53%) (P=.09). 1999;159(19):22832288. Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health. This site complies with the HONcode standard for trustworthy health information: verify here. A one-month trial of medication that reduces stomach acid is often advised. American College of Gastroenterology. Feb. 5, 2022. Doctors consider it a functional disorder, which means its not necessarily caused by a specific disease. MPorro
A side-effect of some medicines can cause dyspepsia: There are various other medicines which sometimes cause dyspepsia, or make dyspepsia worse. Mean dyspepsia scores. The combination of psychologic symptoms, motility dysfunction, infection, and nonulcer dyspepsia may be best understood as a complex interaction of factors. Some people feel that certain foods and drinks may cause the symptoms or make them worse. EKeane
Among the CagA-positive patients, there was no difference in the change in dyspepsia score between those with successful eradication (27131, 25143, 5142, and 3145) and those with persistent infection (50145, 81137, 53141, and 47151) at any time. MLonardo
BSLin
AGuan
Patient meets the following criteria for at least 12 weeks (which need not be consecutive) within the preceding 12 months: Persistent or recurrent symptoms (pain or discomfort centered in the upper abdomen), No evidence of organic disease (including on upper endoscopy) that is likely to explain the symptoms, No evidence that dyspepsia is relieved exclusively by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel syndrome), Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow), Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 enzyme inhibitors. To prepare for your appointment, try to: Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. 2021; doi:10.3389/fmicb.2021.630852. Presented in part at the annual meeting of the American Gastroenterological Association, San Francisco, Calif, May 19-22, 1996. The change in dyspepsia score was calculated by taking the difference in the score at baseline from the score at 1, 3, 6, and 12 months (negative changes in the dyspepsia score indicated improved symptoms, while positive changes indicated worsened symptoms). Both H pylori infection and dyspepsia are common, and many patients with dyspepsia are infected with H pylori. Chey WD, et al. Accessed Jan. 31, 2022. If you have non-ulcer dyspepsia, the inside of your gut looks normal. This content does not have an English version. TTalley
The cause of irritable bowel syndrome is not known. However, at one year, the improvement in symptoms was not statistically significant in two of the studies.20 [SOR B, inconsistent findings from RCTs] Results from these studies were not combined because the interventions were quite different. Establishing the diagnosis of peptic or duodenal ulcer greatly clarifies the treatment approach. Peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer must be excluded. CDMelton
CO'Morain
Accessed Jan. 31, 2022. Non-ulcer stomach pain can cause signs and symptoms that resemble those of an ulcer, such as pain or discomfort in your upper abdomen, often accompanied by bloating, belching and nausea. All Rights Reserved. When signs or symptoms do occur with H. pylori infection, they are typically related to gastritis or a peptic ulcer and may include: Make an appointment with your health care provider if you notice any signs and symptoms that may be gastritis or a peptic ulcer. Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press. The amount of acid in the stomach is normal. Epub 2017 Dec 4. ARSchleck
Seek immediate medical help if you have: There is a problem with The following are some theories as to possible causes: Strictly speaking, non-ulcer dyspepsia is a diagnosis that is made only when no other cause can be found for the symptoms (such as an ulcer). Prior to enrollment, patients had been referred to the gastrointestinal clinic for evaluation at San Francisco General Hospital, San Francisco, Calif. See permissionsforcopyrightquestions and/or permission requests. National Institute of Diabetes and Digestive and Kidney Diseases. Helicobacter pylori (adult). Studies have shown that symptomatic improvement is 45 to 50 percent greater with cisapride, domperidone, or metoclopramide therapy than with placebo.4,28 [Reference 28: SOR A, systematic review of limited-quality studies] However, the studies have been of poor quality. An ache or burning pain in your stomach (abdomen), Stomach pain that may be worse when your stomach is empty, Severe or ongoing stomach (abdominal) pain that may awaken you from sleep, Bloody or black vomit or vomit that looks like coffee grounds. A 2 test with a Fisher exact test was used for comparison between proportional data.28 All tests were 2-tailed, and P values less than .05 were considered statistically significant. For every 15 patients with nonulcer dyspepsia in whom H. pylori is eradicated, one fewer patient has dyspepsia a year later.32 [SOR B, systematic review of inconsistent or limited-quality studies] Another study found a small increase (7 percent) in the likelihood of treatment success with H. pylori eradication.33 [SOR B, systematic review of inconsistent or limited-quality studies], More studies are needed to resolve the conflicting study results and to determine whether, as some investigators claim, a modest benefit for H. pylori eradication may be cost-effective.31 Eradication regimens are reviewed elsewhere.34. Three (8%) of 40 patients in the placebo group and 31 (71%) of 44 patients in the omeprazole and clarithromycin group had complete eradication of H pylori (P<.001). Peptic ulcer disease. H. pylori may also be spread through contaminated food or water. The muscles in the stomach wall may not work as well as they should. Patients and Methods
All Rights Reserved. Pain that radiates to your jaw, neck or arm. Continuous variables are presented as meanSD. CLong-term prospective study of, Lazzaroni
A test to detect the H. pylori germ (bacterium) may be done. Functional or non-ulcer dyspepsia is common and can be long-lasting. A more recent article on functional dyspepsia is available. All Rights Reserved. B
The groups were well matched for demographic and laboratory parameters, with the exception of a higher mean serum alanine aminotransferase level in the actively treated group (Table 1). To explain the symptoms of nonulcer dyspepsia more fully, researchers have focused on several key factors: motility disorders, nonmotility disorders (including H. pylori infection), and psychosocial factors. Risk factors for H. pylori infection are related to living conditions in childhood, such as: A peptic ulcer is a sore on the lining of your stomach, small intestine or esophagus. WLThe treatment of. Your doctor may recommend lifestyle changes to help you control your functional or non-ulcer dyspepsia. Furthermore, patients with persistent, Patients with nonulcer dyspepsia should not routinely be treated for. information and will only use or disclose that information as set forth in our notice of In general, the trials included patients with documented H. pylori infection, used typical dual or triple therapy for H. pylori infection (i.e., antisecretory therapy plus antibiotics), and evaluated dyspepsia at three and 12 months. The guidelines outlined in the Maastricht European consensus report25 recommend endoscopy for patients older than 45 years, whereas the American Digestive Health Foundation26 recommends endoscopy for patients with dyspepsia who are older than 50 years. Effect of treatment of, Sung
In the present study, we enrolled patients in whom an empiric trial of a histamine2-receptor antagonist had failed and in whom peptic ulcer disease and gastroesophageal reflux disease had been excluded. DYLew
JHPeterson
The studied interventions included psychotherapy, psychodrama, cognitive behavior therapy, relaxation therapy, and guided imagery or hypnosis. Copyright 2022 American Academy of Family Physicians. The dyspepsia score was calculated by summing the mean scores for 5 symptoms (nausea, abdominal pain, abdominal bloating, abdominal burning, and pain after eating). 2019; doi:10.3748/wjg.v25.i37.5578. Therefore, H2RAs are preferred, because of their lower cost.28 One review4 noted that most studies have used higher H2RA dosages than those available in over-the-counter formulations, with improvement occurring in approximately 25 percent more patients treated with H2RAs compared with placebo. Not surprisingly, nonulcer dyspepsia is responsible for substantial costs to the U.S. health care system (direct medical costs) and to society (e.g., lost time from work, diminished work productivity).6 A better understanding of this condition and its management can improve patient care and decrease unnecessary medical expenditures. Stress from life events also has been correlated with these symptoms and has been linked to exacerbations of nonulcer dyspepsia.1 In addition, the condition has been linked to the symptoms of irritable bowel syndrome (despite the emphasis on lower versus upper gastrointestinal tract symptoms), an illness known to be connected to stress.21. Kang
What are the treatment options for non-ulcer dyspepsia? information highlighted below and resubmit the form. You may also learn ways to reduce stress in your life in order to prevent functional or non-ulcer dyspepsia from recurring. The diagnosis of dyspepsia is challenging because patients often exhibit changing symptoms, and because characterization of the symptoms provides little information about the nature of the underlying physiologic abnormality.22,23. What treatment you receive depends on your signs and symptoms. A popular, although unproved, management strategy has been to screen dyspeptic patients with a serum enzyme-linked immunosorbent assay for H pylori.31-33 Patients with positive results are then treated for H pylori and are followed up clinically. All rights reserved. An organic cause, such as duodenal ulcer, is found in only about 40 percent of these patients.1 Hence, dyspepsia is considered to be functional, or idiopathic, in as many as 60 percent of patients (Table 1).24 The Rome II criteria provide an updated definition of nonulcer dyspepsia (Table 2).5 Symptoms usually are categorized as ulcer-like (i.e., burning sensation, relief with antacids and histamine-H2 blockers or proton pump inhibitors), dysmotility-like (i.e., nausea, bloating, early satiety, anorexia), or unspecified.5. People often get H. pylori infection during childhood. Because eradication of H pylori in patients with peptic ulcer disease successfully reduces the recurrence of ulcers and improves symptoms,21-26 it is possible that eradication of H pylori will similarly improve symptoms in patients with nonulcer dyspepsia. information is beneficial, we may combine your email and website usage information with I have these other health conditions. J, Rokkas
If you are infected with H. pylori, the first treatment usually tried is to clear the H. pylori infection. YBurette
In 2 of these studies, however, there were only about 20 patients randomized to each study arm, with even fewer completing the study.5,6 Another study did not have a control group and had an extremely high reinfection rate, suggesting that H pylori was not truly eradicated.4 Most importantly, none of these 3 studies had a true untreated, placebo group, and none provided data on an intention-to-treat basis.